
Yesterday, my sister (who lives in the Bentleigh district and South Metro region) gave me an interesting pamphlet that was slipped in her letterbox. Authorised (in teeny tiny type at the back) by Margaret Tighe for Right To Life, the three-fold leaflet makes a lot of misleading and outright false claims about the Voluntary Assisted Dying legislation. It needs debunking, and I’m here to do just that.


I’ll take the text in the order it should be read, opening with:
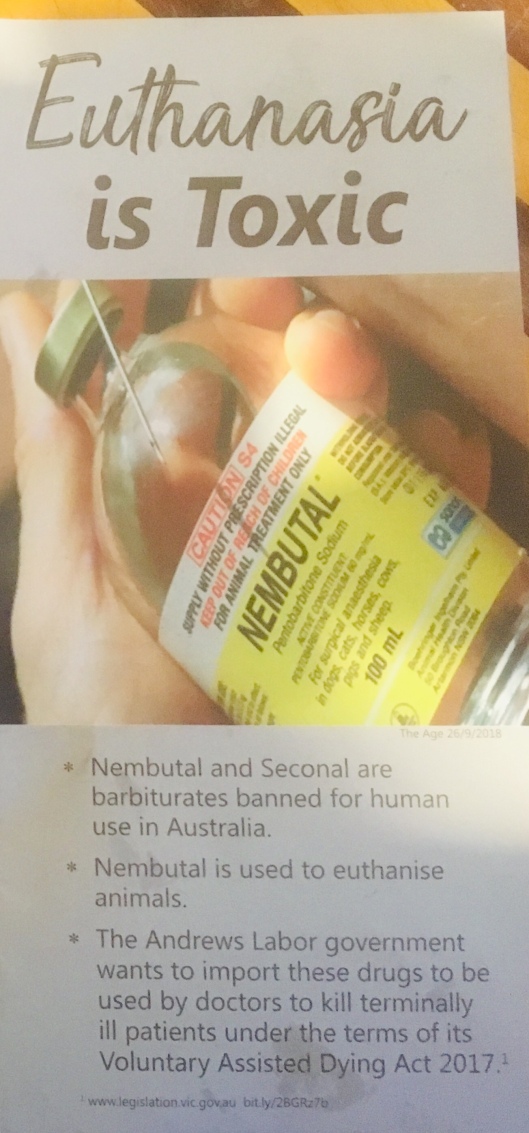
Four claims here, three true but incomplete, and one false:
1) euthanasia is ‘toxic’ – the compounds used are capable of causing death; that’s the prescribed intention.
2) pentobarbital and secobarbital (the generic names for these drugs) are barbiturates, a drug class used for sedation and anxiety management before the introduction of benzodiazepines, which have a far wider therapeutic window, which means they’re safer in higher doses. Barbiturates are the drug class of choice for assisted dying, because they’re painless, generally well tolerated (i.e. unlikely to be vomited up, cause coma without death), available in oral and IV forms, and invariably lethal in high doses.

The NT Rights of the Terminally Ill Act 1995 allowed terminally ill adults, after medical review by three physicians (including a specialist and a psychiatrist), to access physician-assisted suicide via a device created by euthanasia-advocate Dr Philip Nitschke – the Deliverance Machine (above) released a fatal dose of barbiturates into the patient’s bloodstream if they responded ‘yes’ to a series of questions on the attached laptop.
3) Once a schedule 4 drug (available only by prescription), pentobarbital and secobarbital were rescheduled for animal-only use in conjunction with the Liberal Federal government’s Euthanasia Laws Act 1997, which blocked the NT legislation from being used again. The rescheduling was specifically to prevent the use of these drugs for being used for this purpose; they were not banned outright, as the populace would be outraged if vets could not quickly and painlessly euthanise animals.
4) The classification of medications and poisons is federally mandated, and cannot be overruled by a state government – any pharmacist, doctor, or other regulated health professional who documents, distributes, prescribes, or administers medications outside these regulations would have their registration reviewed, which is why you can’t just ask a vet for a dose to help your aunt Vi die peacefully.
The 2017 Victorian legislation does not mention any class of drug, let alone the names of any specific medications, referring only to a compound, which would be individually prescribed by the primary doctor in each case.

Page two is factually correct in all respects :
1) although some 80% of Victorians support the right of competent, dying adults whose suffering cannot be eased to have assistance to die, the legislation did not pass with an overwhelming majority
2) while the word ‘kill’ is emotive, it’s true that the VAD law is a significant change for Victoria
3) while ethicists debate the distinction between withholding life-extending treatment and withdrawing them, there absolutely is a qualitative and real difference between withdrawing an intervention that is prolonging life (like a ventilator) and introducing an agent with the intent of expediting (inevitable, imminent) death
4) and 5) the problem here is that assisted dying is being artificially connected to suicide, for while it is certainly true that VAD is the deliberate ending of a person’s life at their behest and (almost always) by their hand, it is not suicide. How can I say that? Here’s a list of factors that contribute to and reduce suicidality (via The Black Dog Institute)


None of these relates to the situation of someone seeking Assisted Dying. And it’s not just Black Dog – Lifeline’s advice also doesn’t apply to this circumstance:



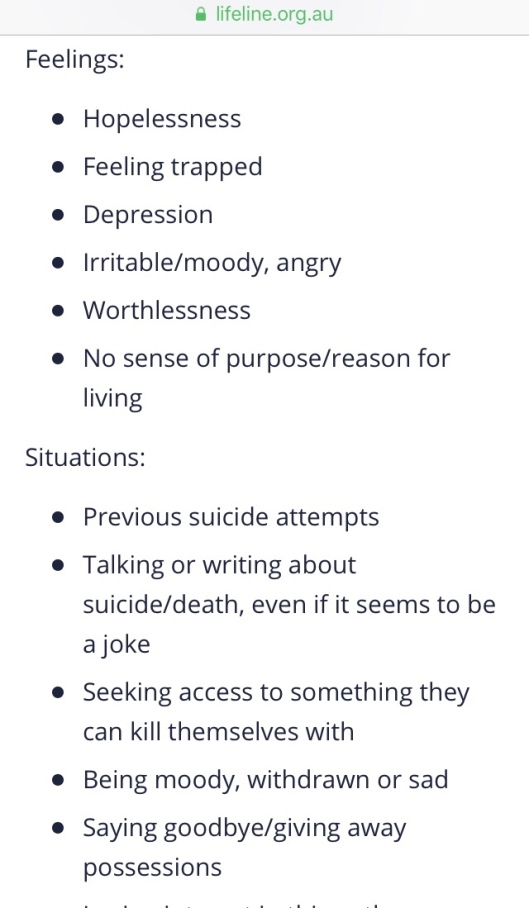

Suicide is a real and important issue; as is oft said, it is a permanent solution to a temporary problem – assisted dying is about reducing the length of time someone whose death is inevitable and imminent experiences unbelievable suffering, after other options have been exhausted.
There are four claims and two quotes on page three:

While the claims here are true, their juxtaposition presents an argument, without requiring the author/s to do the work of making it valid.
1) Premier Andrews and Health Minister Hennessy correctly state that the VAD legislation is the safest of any kind in this area
2) the phrase ‘out of control’ is undefinable, unsourced, and relates to the very different legislation of Europe
3) while substantively true, this implies that our vulnerable people are at risk of being killed without their consent, something not possible here
4) the UK vote did not have our legislation to take into account.
Interestingly, there is no mention of Oregon, where similar (but less well safeguarded) laws to Victoria’s have been in place for two decades, with no claims of anyone’s life being ended without consent.
Next we see a whole two members of the British parliament quoted to support Ms Tighe’s position; to give some context to those quotes, there are currently 791 Lords, including 92 hereditary peers and 26 Anglican bishops; there are 650 members of the House of Commons.
To page four:

Some doctors absolutely oppose assisted dying, as do some nurses. Other things some medical doctors oppose include contraception, evolution, easing the suffering of the dying, and the idea that the earth is round.
Other doctors, and nurses, support it, here and overseas.
On to page five:

There is so very much wrong here.
1) This is a distortion – people with a mental illness that impairs their competency may not, under any circumstances, access VAD in Victoria. However, just as a competent person with (for example) well-managed depression can drive, vote, enter into contracts, run for office, and make other decisions about their health, a competent person with a previous or controlled mental illness can also pursue VAD.
2) The requirements for competency do not change in the presence of other conditions. A person with suicidal depression can be sectioned under the Mental Health Act and required to have life-saving intervention, including dialysis, against their will.
In addition to this, one of the qualifying requirements is that the suffering cannot be relieved in a way the patient seems tolerable, with two physicians assessing their position and condition – ceasing treatment to change a life-limiting condition to a terminal one would trigger a mental health review and likely undermine competency.
Also, note that the rate of assisted suicide uptake in Oregon is around 0.4%, despite a similar rate of chronic disease and mental ill-health, plus health care inequity that doesn’t exist here. There is no requirement there for suffering, only a six-month life-expectancy, but this scenario drawn by Right To Life has not emerged – most of us want to live, regardless of how hard that living is, and unless you’ve experienced or witnessed it, it’s near impossible to appreciate just how difficult living with chronic illnesses can be.
The last page is incontrovertible: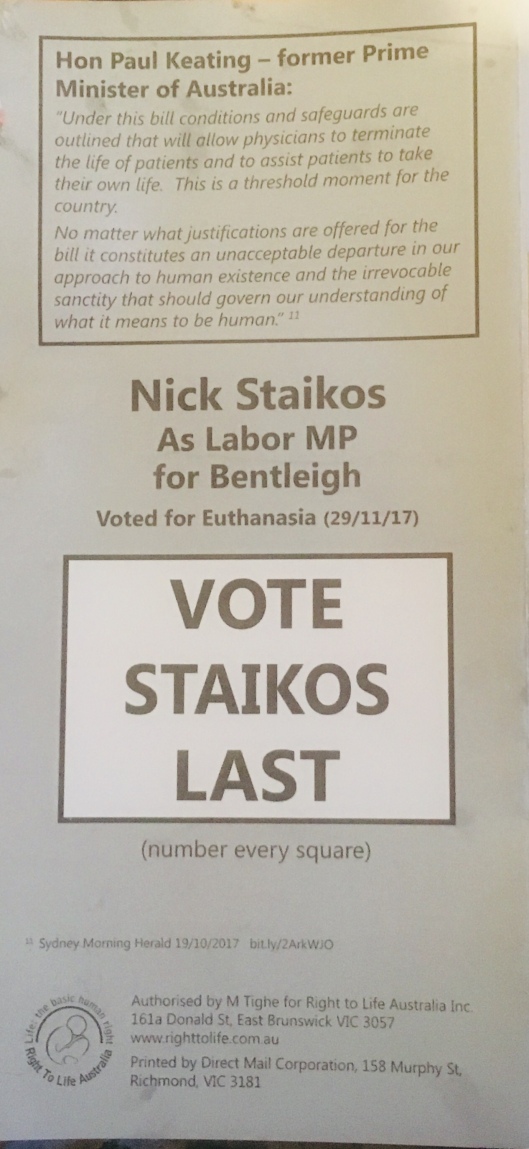
Catholic Mr Keating does oppose Assisted Dying, and Mr Staikos did vote in favour of the bill, so this is all accurate.
